- A new scientific truth does not triumph by convincing its opponents, but rather because its opponents eventually die, and a new generation grows up that is familiar with it. - Max Planck 1858-1947
- A new scientific truth does not triumph by convincing its opponents, but rather because its opponents eventually die, and a new generation grows up that is familiar with it. - Max Planck 1858-1947
José Lévesque installed commercial wireless telephone stations from 2001 to 2009. The resident of Saint-Colomban (Quebec) says in late 2005 he suddenly developed an intolerance to the radiofrequency (RF) microwaves emitted by these devices. "At first it pinched in my ear when I phoned. Even though I used a good headset, I was dizzy and my ears were ringing. Then I woke up one morning and walked as if I was drunk and heard a tone, like a smoke detector in my ear."
Lévesque finally quit his job in 2009 when his so-called electrohypersensitivity (EHS) worsened. "Today, my face goes numb, my head aches and if I continue to expose myself to RFs, I even get nose bleeds or blood vessels burst in my eyes. It happened to me in a hospital with wireless phone and Wi-Fi antennas! We used to laugh about it at work: I could tell my colleagues when their cell phone was about to ring because the entering signal hurt my head." But it is no laughing matter: "Since smart meters were installed in my neighbourhood in January 2013, my headaches are constant."
In today's wireless world, about 3% of Canadians have received the controversial diagnosis of environmental sensitivity — EHS and/or Multiple Chemical Sensitivity (MCS) — "and many more are somewhat sensitive to traces of chemicals and/or electromagnetic phenomena in the environment", wrote the Canadian Human Rights Commission (CHRC) in the report Medical Perspectives on Environmental Sensitivities, published in 2007. EHS is a controversial condition characterized by various non specific symptoms believed to be triggered in some people by very low exposures to electromagnetic fields most of us tolerate. Despite the lack of medical consensus around it, CHRC also adopted a policy aiming to stop discrimination against the environmentally hypersensitive, as many of them lose their job and are referred to psychologists, when they are not sent to psychiatry.
And just recently, on June 17 2015, the Canadian Parliament's Standing Committee on Health (HESA) published a historic report making 12 recommendations to the Canadian government after holding public hearings on Health Canada's Safety Code 6 on human exposure to electromagnetic fields. Entitled Radiofrequency Electromagnetic Radiation and the Health of Canadians, the report calls notably on Canada to "continue to provide reasonable accommodations for environmental sensitivities, including electromagnetic hypersensitivity, as required under the Canadian Human Rights Act". It also recommends funding research into testing, diagnosis and treatment of EHS and its possible impacts on health in the workplace and to ensure medical guidelines and continuing education be updated based on the latest scientific evidence. The report was timely as cutting edge evidence on EHS and MCS was presented by world-class experts last May 18 in Brussels, at the Belgian Royal Academy of Medicine. The 5th Congress of the Paris Appeal's theme was Environmental idiopathic intolerance: what role for EMFs [Electromagnetic fields] and multiple chemicals. The conference's Powerpoint presentations and videos are all available on the conference's website and you can also view its press conference and exclusive interviews on our Youtube channel (and please excuse my amateurish first attempt at producing videos with an iPad).
I was invited to cover this conference by its organizer, Dr Dominique Belpomme, who treats more than 1,200 people with EHS and/or MCS. It is Europe's largest single cohort of environmentally ill patients presently studied. Head of the Association for research on anti-cancer therapies (ARTAC) and of the European Cancer and Environment Research Institute (ECERI), Belpomme recently developed a new method of diagnosing and treating EHS, a condition which he says is not psychosomatic, as many people (even physicians) believe. "We have created an independent international working group to ask the World Health Organization (WHO) to recognize chemical and electromagnetic hypersensitivity in the International Classification of Diseases (ICD) on the basis of new scientific data," he said in an interview. WHO publishes research priorities and public health reports related to EMFs and other pollutants, but does not fund such research. Environmental and public policy consultant Cindy Sage, co-Editor of the BioInitiative Reports summing up what's known about EMF health effects, said there is now so much evidence of the health risks of long-term, low-level exposures to EMFs that if we ignore it, EHS will become a larger and larger and more costly global public health problem. The evidence is sufficient to change public health standards and adopt exposure limits which are biologically based. «We needed them yesterday but we'll settle for today.''
Dr Belpomme added that WHO's December 2005 backgrounder on EHS urgently needs to be updated. This report recognized that EHS causes "long lasting symptoms and severe handicaps", but added that it is not a medical diagnosis and that there is no conclusive proof that it is triggered by EMFs. "The majority of studies indicate that EHS individuals cannot detect EMF exposure any more accurately than non-EHS individuals, WHO wrote. Well controlled and conducted double-blind studies have shown that symptoms were not correlated with EMF exposure... EHS has no clear diagnostic criteria and there is no scientific basis to link EHS symptoms to EMF exposure."
Conflicts of interests

But several experts we interviewed in Brussels said the studies quoted by the WHO were designed to fail. First because it is very rare, even in EHS patients, that people can instantly feel EMFs. Second, because those studies, which are generally performed by scientists linked to the electrical or telecommunications industries, ignore the many types of EMFs and ways they provoke EHS symptoms minutes or hours after exposure. In fact, "certain provocation studies showed changes in pupils, in cardiac rhythms, erythrocite (red blood cell) damage and impaired glucose metabolism in the brain after exposure to EMFs", Swedish oncologist and epidemiologist Lennart Hardell said in Brussels. Such data was reflected in 2012 when the Austrian Medical Association became world's first national physicians' organization to publish a Guideline for the diagnosis and treatment of EMF related health problems and illnesses (EMF syndrome). It stated: "In May 2011, the Parliamentary Assembly of the Council of Europe adopted [via Resolution 1815] the report The potential dangers of electromagnetic fields and their effect on the environment (PACE 2011). The report calls for a number of measures to protect humans and the environment, especially from high-frequency electromagnetic fields. One of the recommendations is to "take all reasonable measures to reduce exposure to electromagnetic fields, especially to radio frequencies from mobile phones, and particularly the exposure to children and young people who seem to be most at risk from head tumours."
Electrical engineer Emilie van Deventer, who heads the WHO International EMF Project, told us by email her team is currently reviewing the international scientific literature on RF health effects. "A monograph in the series of WHO Environmental Health Criteria will be published next year. This will include the review of publications on electromagnetic hypersensitivity."
But many people doubt the new monograph will substantially change WHO's position. WHO's EMF Project has been mired in conflicts of interests from the start, charges brain cancer survivor Lloyd Morgan, who represents patients as a Director of the American Central Brain Tumor Registry. A doctor of electrical engineering, van Deventer once headed a research chair on EMFs at the University of Toronto financed by wireless giants Bell Canada and Nortel. "To my knowledge, she has little, if any knowledge about biology, medical practice or public health", Morgan wrote us, adding she replaced her mentor Michael Repacholi, a former Health Canada scientist and consultant to electric utilities. Repacholi founded WHO's International EMF Project in 1996 with industry funding "in a money laundering" scheme, Microwave News revelead in 2006. He arranged for the money to be sent to his former employer, the Royal Adelaide Hospital in Australia, which later "donated" it to WHO. Repacholi also founded the International Council on Non-Ionizing Radiation Protection (ICNIRP) whose recommended RF-exposure limits are the basis of Safety Code 6 and most other national guidelines. These only consider risks of body heating and ignore non-thermal effects of EMFs from low-level but long-term exposure, such as headaches, insomnia and opening of the blood-brain barrier. "In effect the International EMF Project is industry's mole embedded within WHO", Morgan wrote. Van Deventer did not reply to our requests to comment on this charge.
Many other speakers at the Brussels conference noted scientists who claim EHS is psychosomatic are associated with the electricity and wireless industries. ICNIRP states that its members are independent of commercial interests, but several have been accused of conflicts of interests. Besides Repacholi, the most famous is Anders Ahlbom, professor of epidemiology at the Karolinska Institute and former consultant to the tobacco industry. In 2011 he was forced to resign as a member of the International Agency for Research on Cancer (IARC)'s working group on radiofrequencies. Swedish journalist Mona Nilsson had revealed that he was director of the consulting firm Gunnar Ahlbom AB, founded by his brother and serving telecom firms, Microwave News reported. A few days later, IARC officially classified RFs as "possibly carcinogenic".
Historical conference
Some 160 doctors, scientists, lawyers and other participants attended the Brussels conference to hear 15 international EMF-effects experts (who all spoke in English). In his presentation, Dr Belpomme said brain scans showed many of his EHS/MCS patients suffer from lack of blood flow in the brain (cerebral hypovascularisation) and insisted that physicians must take their stories seriously as the father of medicine Hippocrates recommended. "In the last four years, I have personally examined 1,213 patients and 90% of them are really electrohypersensitive as they meet our three objective clinical criteria: their symptoms are not explained by a known pathology, they appear and are reproducible under the effect of electromagnetic fields, and they regress or disappear when they avoid these waves. Objective blood and urine tests as well as Doppler ultrasounds of the carotid artery show these patients are suffering from brain alterations, especially in the very important areas of the limbic system and the thalamus. Our results need to be confirmed by international studies, but we have sufficient scientific knowledge for governments to recognize the disease." 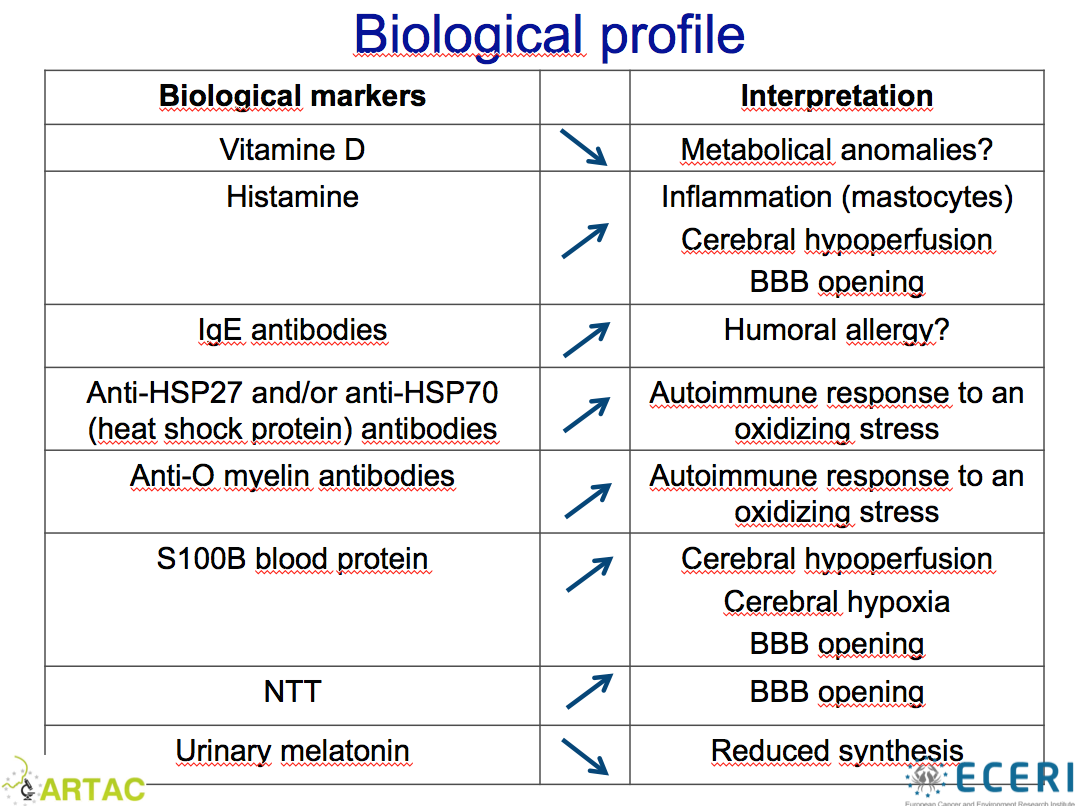
Belpomme found many of his patients have abnormally high levels of histamine (a marker of inflammation), IgE antibodies (a sign of allergy), heat shock proteins HSP27 and/or HSP70 (cellular stress), S100B protein (cerebral suffering) as well as anti-O-myelin antibodies (cellular stress), and lower levels of vitamin D (metabolic anomaly) and urinary melatonin (EMFs halt production of this vital tumor-fighting hormone which regulates our biological clock). Besides the need for lowering EMF exposure as a top priority, Dr Belpomme said promising EHS treatments include using antihistamine medication, natural anti-inflammatories such Ginkgo biloba and especially Fermented Papaya Preparation (FPP) which favors cerebral blood flow and which is also used to stimulate the immune system in AIDS patients, as well as vitamins and minerals which are lacking in people with EHS. (The FPP has reduced by nearly 100% my own back aches - my osteopath is amazed! - and my wife's headaches and sensitivity to perfumes, problems we experienced for 30 years.) Belpomme also noted the treatment must be tailored to each patient's specific biological profile and symptoms. Many of them for example have high levels of heavy metals which are neurotoxic and all metals (worn or implanted) act like antennas capturing radiofrequencies. Belpomme said his study of more than 700 EHS/MCS patients will be published in a peer-reviewed medical journal in 2016.
An old problem exploding

Between 1995 and 2004, several European surveys showed the proportion of people saying they were more or less intolerant to EMFs jumped from 1,5 % in Sweden to 11 % in England. Nordic countries have even recognized EHS as a functional impairment, Swedish neuroscientist Olle Johansson explained at the Brussels conference. Head of the Experimental Dermatology Unit at the Karolinska Institute in Stockholm, and a pioneer in investigating EHS since the 1980s, Johansson notes that while not recognized as a medical diagnosis by WHO, in 2000 EHS was included as a functional impairment in The Nordic Adaptation of Classification of Occupationally Related Disorders (Diseases and Symptoms) to ICD-10 published by the Nordic Council of Ministers representing Norway, Finland, Sweden and Denmark. This report stated that so-called idiopathic (meaning of unknown cause) environmental intolerance encompasses multiple chemical sensitivity (MCS) and electromagnetic intolerance (or el-allergy) which it defined as: "Usually general symptoms (tiredness, nausea, memory- and concentration difficulties etc.) related to use of TV/PC/data-screens, electrical transformers or fluorescent lamps. Symptoms disappear in "non-electrical environments."
But there's nothing new about EHS. It was first diagnosed as microwave syndrome by German physician Erwin Schliephake in 1932. And during the Second World War, radar operators overexposed to RFs were often struck with what was then called microwave illness, Dr David Carpenter explained in Brussels. The former founding dean of Albany (New York) University's School of Public Health, and presently its head of the Institute for Health and the Environment, Dr Carpenter is co-editor with Cindy Sage of the famous independent reports on the health effects of EMFs published in 2007 and 2012 by the BioInitiative Working Group.

According to Carpenter, despite the lack of scientific consensus on its causes and mechanisms, "the evidence is strong enough to declare that electromagnetic hypersensitivity is real; it can even be triggered by a slight shock, but each individual reacts differently. Many people are unaware that it is the cause of their various nonspecific symptoms that have long described as neurasthenia. It is important to design objective tests to determine which patients are truly hypersensitive while recognizing that some symptoms can be psychological in origin. I do think that viewing EHS and MCS as having many things in common is right on. In addition I would add chronic fatigue, fibromyalgia and Gulf War Illness to the list of idiopathic environmental intolerance diseases. He added that we should not only be concerned with the frequency and power of microwaves. "Sudden spikes of frequency transients and harmonics may well be what we should be more concerned about. It's the same phenomenon that occurs with wireless devices such as smart meters that emit very short pulses of high intensity."
Dr Carpenter added that a classroom full of children using laptops hooked up to the Internet with wireless Wi-Fi routers can «generate an enormous level of radiofrequencies (RFs) which may be enough to trigger the development of EHS which will continue for life''. Close to sources of such EMFs, people with EHS typically develop headaches, fatigue, mental dullness, irritability and a general reduction in ability to function. ''Not only are children more vulnerable to every environmental exposure, he said, but if we allow our children in schools, where they are supposed to be learning, to be exposed to an agent that reduces their ability to pay attention and to learn and promotes illness, this is a tragedy, it's foolish and we should act right there to reduce the exposure... A wired computer classroom will not result in [RF] exposure connection, will have the same access to the Internet that every child needs, but to rush ahead and to make everything wireless without contemplating the long-term health effects is unwise.''
Thousands of contradictive studies and the role of industry funding
The non-thermal biological effects of RF EMFs were first recognized by the US government in 1972, in a Naval Medical Research Institute bibliography citing more than 2,300 studies, and in 1986 by the US National Council on Radiation Protection & Measurements. A must read is the 2009 article Cell phone radiation: Evidence from ELF and RF studies supporting more inclusive risk identification and assessment, by former US EPA scientist Carl Blackman - a PDF version can be downloaded by googling its title and choosing the version from www.stichtingehs.nl.)
Physicians' misunderstanding about environmental hypersensitivities is partly due to lack of funding for independent research but there is no shortage for industry-funded scientists. "There are as many studies that failed to detect EHS than studies that have confirmed its existence, Henry Lai, a Research Professor of Bioengineering at the University of Washington and co-editor in chief of Electromagnetic Biology and Medicine Journal, wrote me before my trip to Brussels. Basically, the science of electromagnetic sensitivity is not as strong as most people believe. To make a positive and definitive statement about it is to imitate the same parody that industry is trying to make us swallow by saying that cell phone use is absolutely safe."
Lai, who has been studying the biological effects of EMFs since 1980, speaks from experience. In the early 1990s, he and colleague NP Singh found that very low RF exposures from radar, well below the limits recommended by ICNIRP and Health Canada, damaged DNA. When their discovery was confirmed, cell phone manufacturer Motorola did all it could to discredit them and even tried to have them fired, he told Seattle Magazine. And in 2006, he analyzed funding sources of 326 studies performed on cell phone effects between 1990 and 2006. He found that 73% of industry-funded studies were negative (finding no effect) while 68% of independent studies were positive. Thus even though industry financed only 30% of research on the topic, the overall results were split 50-50. «How could 50 percent all be garbage?", he asked Seattle Magazine. Truth is, he also found 86% of studies showing biological or health effects were funded independently, the Townsend Letter reported. His conclusion: the fact that 50% of overall studies showing effects is significant enough to justify a precautionary approach that minimizes exposures, the
The Brussels keynote address was made by Dr Lennart Hardell, whose research on pesticides since the late 1970s and more recently on cellphone use and brain cancer led to glyphosate (Monsanto's Roundup) and radiofrequencies being classified as possibly carcinogenic. Hardell also said there are many conflicts of interests in the field of EMF research. "Companies have learned that small investments in endowing chairs, sponsoring research programs, hiring professors for out-of-hours projects can produce disproportionate pay-offs in generating reports, articles, reviews and books, which may not be in the public interest, but certainly benefit corporate bottom lines, Hardell said. With the ability to allocate who does the scientific research, the industry also dictates the research itself and how it is interpreted. Industry scientists create ‘counter-evidence' for every alarming discovery so that it can be said that ‘the issue is controversial' and that ‘the scientists have disparate opinions' or that the effect is ‘not conclusively proven'. Thereby doubt is created in the minds of the public and restrictive legislation is delayed. The ‘experts' in this field belong to a number of self-serving committees and organizations. These expert clusters are inevitably linked into industry and industry initiatives. Meanwhile, parents who withdraw their sick child from a school with Wi-Fi are almost treated like criminals." (For more details, read: Institutional Corruption in Dealing With the Risks of Radiofrequency Radiation in the Past 50 Years, by Prof. Franz Adlkofer of the Pandora Foundation.)
David Carpenter adds that the bioelectromagnetics community is dominated by engineers and physicists, not by health professionals. He added these engineers and physicists who are members of ICNIRP developed the international EMF exposure standards based only on avoiding thermal effects ''are not qualified to identify human health effects.''
Why most EHS studies are negative

Igor Belyaev, head of the Laboratory of Radiobiology at the Slovak Academy of Science's Institute of Cancer Research, explained why most EHS studies fail to show some people react to Extremely Low Frequency (60 Hertz ELFs) or to microwaves (MW). "Unfortunately, some reviews and panels in the field of bioelectromagnetics do not include analysis of various biological variables and physical parameters when comparing the data on the ELF/MW effects from different studies. As result, misleading conclusion is made that weak ELF/MW produce no "reproducible" effects. Our analysis suggests that different EMF signals (bandwidth, frequency, modulation, polarization) should be considered with care when studying EMF biological effects including electrohypersensitivity. The data also indicate that durations of exposure and post-exposure are important parameters for setting up the EMF effects. Taken into account the EMF response time kinetics, individual sensitivity, variation in physiology, and dependence on physical parameters it follows that more conditions of exposure should be validated in studies of electrohypersensitivity. Significant body of studies show that ELF/MW effects depend on concentration of divalent metals, free radical scavengers and antioxidants. These studies provide a mechanistic background for treatment of electrohypersensitivity based on chelating divalent metals, reducing ROS [Reactive Oxygen Species turning molecules into free radicals], and balancing vitamins." Besides the frequency/ies of the carrier wave, bandwith (range in frequencies), modulation (the information piggybacking the carrier wave), polarisation, intermittence and coherence of the time of exposure and non exposure, and presence of static magnetic fields and stray currents, EHS symptoms also depend on high body load in heavy metals.
Lawyer and physician George Carlo, who from 1993 to 1999 headed the $28 million Wireless Technology Research Program which linked cell phone use to cancer, wrote by email that he agrees with Belyaev: "The most important determinant of causation is not epidemiological data because that tool is not precise enough to handle a multiple manifestation outcome like EHS. The most important aspect for determining cause and effect in the case of EHS is the biological mechanism of harm. In our experience, it is the Information Carrying Radio Waves — we call them ICRW — that contain the wave forms that trigger sympathetic stress cascades. This means that most problematic for those who suffer from EHS are waves, pushed by power so that there is penetration into the body, that have modulation overlays of time, code, voice or data. Other forms of EMR are usually less efficient triggers of symptoms. Thus, some people are more or less triggered by dirty electricity and powerline-derived fields for example. Also, other forms of ambient fields like loud noises and bright lights are triggers for some people."
Carlo added: "This non-conformity in response also means that studies which use simulated signals — such as those used in the majority of the published challenge studies which are used to support the contention of nocebo effect, psychosomatic triggering or the absence of cause and effect — are measuring exposures that are not likely to trigger the symptoms. They see 'no effect' because they do not have an exposure pattern that is capable of 'causing the effect'. Thus, the majority of the published studies are of limited or no value in determining the causal chain and the medical intervention paths forward. There are efficient screening tools to define whether or not frank 'EHS' is present. These include the laboratory metrics discussed in the article above that require blood or urine samples, as well as precisely targeted HRV assessment, and precise queries designed to define present 'adaptive capacity'. With these data in hand, efficient corrective intervention protocols customized to the individual can be defined and followed. EHS need not be a figurative 'life sentence of debilitation'. It can be managed to the point where a good quality of life can be maintained even in a world awash in wireless signals." (Read our article Electrosensitivity symptoms can be eliminated in 60% of people and significantly reduced in the rest – Dr Brian Clement.)
No psychosomatic, but it's in the head
The Brussels speakers all agreed that while EHS symptoms are not specific to a single disease, they are very rarely psychosomatic. But despite a few high-quality studies that showed in double blind challenges that EHS is truly triggered by EMFs, WHO and countries such as Australia still note that some studies suggest EHS is triggered by the nocebo effect (fear of a substance perceived as noxious). José Levesque replies he told Health Canada and Public Health officials he would volunteer to get tested so they could measure his biological responses to microwaves. They refused. "It's easy to say that this is the nocebo effect when you do not want to test me because you're afraid of being accountable and have to act accordingly, he says. I know that the tests would be full of consequences for me: my symptoms appear 5 to 10 minutes after a Wi-Fi router is turned on close to me, and then I can be sick for three or four days. But if it can help people to realize the dangers of wireless..."
Texas surgeon William J. Rea has heard this kind of story thousands of times since 1974, when the pioneer in environmental medicine founded the Environmental Health Center, in Dallas. The former professor of surgery has treated more than 35,000 MCS and EHS patients, including hundreds of colleague physicians, many of whom he later trained in environmental medicine. In 1991, Dr. Rea published a landmark study of a method of diagnosing electrohypersensitivity. It requires that the patient spend three to four days in a clean, controlled environment to calm his nervous system exhausted by pollutants and eliminate the body's compensations that mask the real triggers of symptoms. More than 700 of his patients underwent a brain tomography showing they had holes or defects on the surface of their brain, indicating a reduction in blood flow or neuronal activity. "It's in the head indeed and I have proof of it!", the 80-year-old physician joked during his Brussels talk, after which he told me that 80% of his EHS patients had been poisoned by mold mycotoxins.
Dr Rea said he challenges EHS patients with different frequencies in a Faraday-cage type room shielded from external electromagnetic fields. ''I just had a rancher who came in who lost 250 of his cattle do to electrical stimulation and we challenged him in the screened room and reproduced the electrical sensitivity on him, reproduced his symptoms. We found the specific frequencies that triggered this, plus the fact that we triggered his symptoms.'' As for treating EHS patients, he finds specific electromagnetic sine waves that are beneficial for each individual, acting as a neutralizing hormonic signal. This technique was developed in the United Kingdom in the 1980s by biophysicist Cyril W. Smith, retired lecturer at Salford University and co-author of the book Electromagnetic Man, and physician Jean Monro, Medical Director of the private Breakspear Hospital based in Hertfordshire. Dr David Carpenter said after the Brussels conference: "I was most impressed by Bill Rea, who I had not met previously. And I bet he is right in his concept that one cannot adequately prove sensitivity without 'unmasking' the environment."
Concerning the nocebo effect theory, Dr Michael Kundi, head of the Institute of Environmental Health at the Medical University of Vienna and who has been studying the health effects of electromagnetic fields since the mid-1980s, said in an interview: «I think the majority of people with electrohypersensitivity didn't even know at first that they were exposed to electromagnetic fields, so I don't think that fear of exposure is the source of the symptoms. It might contribute later to the persistence of symptoms, but the original symptoms in many cases arise without knowledge of the exposure.'' Yet many people in industry and government keep repeating EHS symptoms are due to a phobia provoked by media reports. Prof. Olle Johansson replies: ''This possibility cannot explain why rats and tomato plants and bacteria react negatively [to EMFs], because they don't watch television and read newspapers!''
Other highlights of the Brussels conference
Dr Lennart Hardell added in an interview: "I have followed the litterature (on EHS) and clearly the evidence is there that it's a real disease which is related to exposure to electromagnetic fields. These people need to be recognized as diseased and not like a psychiatric disorder which many doctors by now tend to say, 'Oh this is a psychiatric disease you need to have cognitive treatment'. Instead they need to be carefully taken care of in hospitals. During this conference we are addressing the need for diagnostic criteria and also that EHS should have an ICD code like other diseases because that would facilitate for physicians to treat these patients and take them seriously. Without such a diagnostic code, it's easy to dismiss them. I know the problem is the symptoms can be specific for different individuals and that by now there is no established criteria for establishing the diagnosis. We need to establish the symptoms and also to have biological markers and from that we need to go on to get WHO to accept this as a disease and then establish treatments. I have seen some of the results of Dr Belpomme's research and they are very interesting. These markers may contribute to a diagnosis in the future because he has found several markers are increased in EHS persons. We need also to educate people in society because most people think there is no problem with EMFs and we also need education of medical doctors in the future."
One of Dr Hardell's latest studies, cosigned with Michael Carlberg, recently showed significant increases in the incidence of nervous system tumors of unknown type and in deaths they have caused in Sweden since 2008. The incidence rates increased almost 5% in men and more than 4% in women and the death rates jumped 24% in men and 20% in women. They found both the National Inpatient Registry and Causes of Death Registry indicate a considerable underreporting to the Cancer Register in recent years. "We conclude that the Swedish Cancer Register is not reliable to be used to dismiss results in epidemiological studies on the use of wireless phones and brain tumour risk."
Italian pediatrist Ernesto Burgio, head of the International Society of Doctors for the Environment's scientific committee, explained the role of epigenetics, defined by Wikipedia as "the study of cellular and physiological trait variations that are not caused by changes in the DNA sequence, or, how external environmental factors turn genes on and off and affect how cells read genes". In Europe, child cancers have increased by 50% in the last 25 years and what's surprising is that they are particularly increasing among babies two years and under. Dr Burgio says these increases in cancer and in many chronic diseases such as allergies, type 2 diabetes and even schizophrenia are not due to bad luck, but to how the environment changes our genome, the genetic software which can change DNA which he calls our genetic dictionary. These diseases, he said, "are biological responses to incorrect informations. The environment is changing too fast, our organisms can't keep up." Burgio added that the most important thing we can do is primary prevention: reducing our exposure to EMFs, heavy metals and endocrine disruptors including pesticides. "EMF exposure is increasing everywhere and it's absolutely an underestimated problem. If we start realizing all of this is dangerous, we can begin to reduce exposure, especially in the critical window of the developing fetus, for whom pollution represents a major danger which is even transmitted to other generations by spermatozoa. With primary prevention, we can change the destiny of these children."
Dr Michael Kundi added: ''We have technical solutions but they will not be implemented if we carry on just with the concept that if we just avoid heating (tissues) then we have no problem. So the first step is recognizing non-thermal (biological and health) effects as a real effect and this has not happened in the scientific community in the degree that is necessary.'' Is he optimistic about the future? «I think there is some hope, there is a renewed strength in the scientific community to study EHS seriously, that is from mechanistic, diagnostic and therapeutic standpoints, he replied. And the evidence is increasing that there might be a future for specific diagnostic markers.''
The final word comes from Prof. Olle Johansson of the Karolinska Institute who wrote us in 2012: "In Sweden, EHS is an officially fully recognized functional impairment — i.e., it is not regarded as a disease, thus no diagnosis exists. This is not special for Sweden, the terms "functional impairment" and "disease" are defined according to various international documents. Thus, the first step for a person in Sweden with a functional impairment is to contact the municipality's special civil servant for disability issues, as well as the various handicap organizations and authorities, to achieve accessability measures of various types with the sole aim to have an equal life in a society based on equality (according to the The UN 22 Standard Rules on the Equalization of Opportunities for People with Disabilities - since 2007 upgraded into The UN Convention on Human Rights for Persons with Functional Impairments.
"Persons with the functional impairment electrohypersensitivity have their own handicap organization, The Swedish Association for the Electrohypersensitive (http://www.feb.se; the website has an English version). This organization is included in The Swedish Disability Federation (Handikappförbundens SamarbetsOrgan; HSO; http://www.hso.se; the site has an English short version). As a consequence of this, The Swedish Association for the Electrohypersensitive receives an annual governmental subsidy. An impairment is - by definition - not defined by someone else or proven by certain tests, etc. The impairment is always personal (private) and develops when in contact with an inferior environment. Remember that functional impairments are only based upon each individual's impaired accessability to - and contact with - an inferior environment (cf. the UN), thus, there is actually no need for any "recognition" in local laws. In Sweden, the former Minister of Health and Social Affairs, Lars Engqvist - as a member of the previous government - anyhow gave his "approval" in a letter dated May, 2000. He also made it clear in his response that for EHS persons there are no restrictions or exceptions in the handicap laws and regulations. Thus, these laws and regulations are to be fully applied also for EHS persons.]
"Treating members of the community equally is not something that should be done as a favour; nor is it something that any parliament or government should politely request other inhabitants to provide others with. Equality is not something to be done "out of the goodness of one's heart". It is something one does because it is expected of every citizen, because inaccessibility and discrimination are prohibited by law. Thus, it is not alright to deliberately make your symptoms worse. The electrically hypersensitive must therefore, in every situation and by all available means, demand respect¸ representation and power. They shall very clearly reject all approaches which reflect a mentality of "feeling pity for them" or "caring for them". Inaccessibility is not a personal problem. It is a problem for society. Inaccessibility is not about attitudes. It is about discrimination. And discriminatory actions and conduct shall not be dealt with by well-meaning talk about treatment. Discrimination is already illegal!"
And at the 5th Paris Appeal press conference, he concluded: «Of course all of us want to be wrong, we want [EMFs] to be completely safe, we want to be able to tell parents that it was OK to go wireless, but then or course a huge proportion of the scientific literature all at the same time needs to be wrong and we are talking about thousands and thousands of papers that are already published. And more are coming, per week it may be 20, 25 papers arriving in my computer... Then of course one has to remember that very many investigations and results actually started with a single scientist. Then we could be right, and we would be sad.''
For more information, see the full 5th Paris Appeal program and presentations.